ECG Basics

An electrocardiograph (ECG) is a quick and fairly simple tool that records the electrical activity of the heart . It uses electrodes placed on the surface of the skin to record changes in voltage over time as a tracing across the page. Because it is only a surface recording it is non-invasive and painless.
An ECG can be recorded for many different reasons. It is often used when a patient has symptoms such as chest pain, palpitations, syncope or loss of consciousness. It can diagnose a range of cardiac arrhythmias, and can show signs of systemic diseases.
Basic ECG interpretation includes checking its quality and describing its waves, segments and intervals. This descriptive information can then be used to analyse the rhythm, axis and presence of ischemia or specific diseases. Each ECG should be interpreted in the clinical context of that patient at that time, and it should be compared to their baseline ECG if possible.
Waves
An ECG wave is a deflection (i.e. a bump, spike or ripple) that is recorded by the ECG machine when the surface voltage changes. Just like ocean waves, ECG waves come in many different shapes and sizes.
Positive and negative waves
Quiz
Let's start by describing ECG waves as positive, negative or biphasic.
Positive waves are above the baseline of the ECG.
Negative waves are below the baseline (upside down).
If a wave is both positive and negative, it can be called biphasic.
Naming Waves
ECG waves are named using letters of the alphabet.
The first wave of each beat is called the P wave. The P wave is usually small and hard to see.
After the P wave there is a tight group of waves called the QRS complex.
The first wave of the QRS complex is named a Q wave, if it is negative. Q waves are always negative.
A positive wave in the QRS complex is called an R wave. It is often tall and sharp.
If there is a negative wave after an R wave, it is called an S wave. S waves are also always negative.
The T wave occurs after the QRS complex.
Naming complexes
An ECG complex is a tight group of waves.
The QRS complex is the main ECG complex. It is named by the Q, R and/or S waves that make it up (they are not always all present). For example, if there is no S wave the complex can be named a QR complex. Or, if there is no R wave it can be named a QS complex.
Describing complexes
Just like waves, QRS complexes can also be described as positive or negative. This will be useful for working out features like the cardiac axis later on.
Positive complexes are overall taller above the baseline than below.
Negative complexes are overall more below the baseline than above.
If a complex is equally positive and negative, it can be called isoelectric or equiphasic.
Segments
ECG segments are the gaps between two waves. They are generally named by the waves on either side of them.
The PR segment is the gap between the end of the P wave and the start of the QRS complex.
The ST segment is the gap between the end of the QRS complex and the start of the T wave.
Intervals
ECG intervals are periods of time that include at least one wave and segment. They are generally named by the waves at either end.
The PR interval includes everything from the start of the P wave to the start of the QRS complex.
The QT interval includes everything from the start of the QRS complex to the end of the T wave.
The RR interval includes everything from one R wave up to the next R wave.
Wave Origins
Core Refs
- John Hampton and Joanna Hampton (2019) 1 The ECG made very easy indeed. The ECG Made Easy, 9th Edition (Book)
- Northern Sydney (2017) Northern Sydney 2017.2. Doctors Writing (Website)
- (2006) ECG Physiology 2006-1. EDvivas for vivas (Website)
{kind=link}
Examples
Depolarisation
Heart muscle contraction is triggered by an electrical event called depolarisation. This can be detected by electrodes on the surface of the skin. If the patient is relaxed so that skeletal muscle interference is kept to a minimum, the ECG can show a clearer picture of cardiac electrical activity.
Depolarisation is the first event of the cardiac action potential. Heart muscle cells are all electrically linked by intercalated discs, which allows action potentials to travel from one cell to another.
Positive ECG waves occur when depolarisation spreads towards a positive electrode. Conversely, negative waves occur when depolarisation spreads towards a negative electrode.
After depolarisation, the process of resetting the cells to their resting state is called repolarisation. This generally occurs in the opposite direction to depolarisation.
The Cardiac Conduction System
The cardiac conduction system shows us how depolarisation spreads through the heart.
- The Sinoatrial (SA) Node: a cluster of specialised cardiac cells (not nerves) that spontaneously depolarise at a rate between 60-100 beats per minute. It is found near the entrance of the superior vena cava in the right atrium. It is also known as the Sinus Node.
- Internodal tracts: also known as interatrial pathways, there are multiple routes that the wave of depolarisation can travel from the SA node to the AV node.
- The Atrioventricular (AV) Node: a cluster of cells found at the interatrial septum. Because the atria are electrically isolated from the ventricles, the AV node is the only bridge between these two regions of the heart. The AV node spontaneously depolarises at a rate of 40-60 beats per minute.
- The Bundle of His: the main conduction highway from the AV node down through the ventricles.
- Bundle Branches: the Bundle of His divides into left and right branches.
- Fascicles: the Left Bundle Branch is so large (because the left ventricle is so large) that it further divides into Anterior and Posterior Fascicles.
- Purkinje fibres: these specialised fibres spread conduction through the heart muscle.
Explaining waves
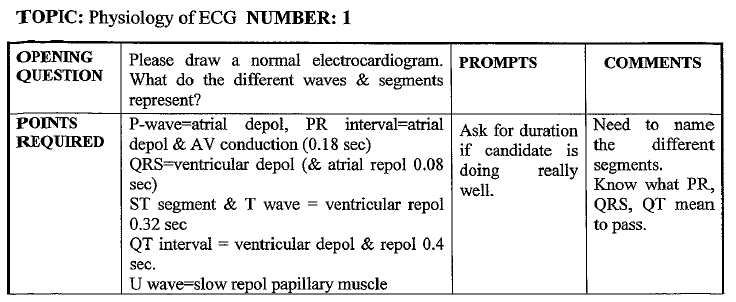
The P wave represents atrial depolarisation. In the normal heart, each beat starts at the SA node but it is so small that there is no change on the ECG (it is electrocardiographically silent). When the impulse leaves the SA node and travels through the atria it makes the P wave appear.
When the impulse reaches the AV node, there is a delay before it enters the ventricles. This delay allows atrial contraction to finish. It makes up part of the PR segment on the ECG. The total time taken within the atria including everything from the SA node to leaving the AV node is the PR interval.
The QRS complex represents ventricular depolarisation. Once the impulse has left the AV node it enters the ventricles and their main conduction highway, the Bundle of His. The impulse races down this bundle and into the left and right bundle branches, through the fascicles, to the Purkinje fibres and through the myocardium.
After the ventricles are depolarised they will contract then repolarise (reset) ready for the next beat. On the ECG this normally produces a flat ST segment then a T wave. The total ventricular time is the QT interval.
Variations
Tall depolarisation waves can suggest larger amounts of heart muscle to depolarise (i.e. atrial or ventricular hypertrophy).
Short depolarisation waves can suggest a barrier between the heart and the surface ECG electrodes, e.g. pericardial effusion.
Narrow waves suggest fast (normal) conduction. For example, narrow QRS complexes suggest that the rhythm origin is supraventricular and the heart is using the normal conduction highways through the ventricles.
Wide waves suggest that conduction is slower than normal. For example. wide QRS complexes suggest that depolarisation is NOT spreading through the ventricles via the normal conduction highways. This could be due to a ventricular arrhythmia or a conduction block.
Segments can be described as isoelectric (flat), elevated or depressed. Isoelectric means flat, elevated is above the baseline and depressed is below the baseline.
Intervals can be normal, short or long. Short intervals can suggest conduction shortcuts such as accessory pathways or genetic ion channel disorders. Long intervals suggest conduction delays.
Leads and electrodes

Did you know that people often use the term lead to mean two different things?
First, there's the 12 leads of the ECG, which are like different channels or views of the heart. Each channel records electrical activity in a single direction. Having 12 different views lets us know more about how electricity moves through the heart in 3 dimensions. Common lead names include I, II, III, aVR, aVL, aVF, V1, V2, V3, V4, V5 and V6.
Then there's the 10 electrodes that are placed on the skin to record the ECG. These are also called leads by some people. Each lead compares two or more electrodes to make the trace. Common electrode names include LA, RA, LL, RL, V1, V2, V3, V4, V5 and V6.
To prevent ongoing confusion, let's just use the term lead for a channel of ECG recording. This means that a standard 12-lead ECG is recorded using 10 electrodes.
Core Refs
- John Hampton and Joanna Hampton (2019) 2. The basics: the fundamentals of ECG recording, reporting and interpretation. The ECG Made Easy, 9th Edition (Book)
Electrodes
ECG electrodes must be placed on the skin in very specific locations.
The first 4 electrodes are placed on the limbs. They are named after each limb, including Left Arm (LA), Right Arm (RA), Left Leg (LL) and Right Leg (RL).
There are 6 other electrodes that are placed on the anterior chest wall (also known as the precordium). They are named V1-V6.
- V1 is placed in the 4th intercostal space at the right sternal border.
- V2 is placed at the same level on the left sternal border.
- V4 is then placed in the 5th intercostal space at the mid-clavicular line.
- V3 is half way between V2 and V4.
- V5 is on the same level as V4 but at the anterior axillary line.
- V6 is also at this level but in the mid-axillary line.
The V4 electrode is often placed before V3, because it helps to locate the site for V3.
Limb leads
The limb electrodes are used to record 6 limb leads on a 12-lead ECG. These limb leads are named I, II, III, aVR, aVL and aVF. They each view the heart from a different direction in a frontal plane.
- Lead I looks at the heart horizontally from right to left. It compares the RA (-) electrode to LA (+).
- Lead II looks at the heart diagonally from the right shoulder to left foot. It compares the RA (-) electrode to LL (+).
- Lead III looks at the heart diagonally from the left shoulder to left foot. It compares the LA (-) electrode to LL (+).
The next 3 leads are called augmented leads. They are calculated from leads I, II and III with a mathematical transformation to make them large enough to see clearly.
- Lead aVR looks from the center of the heart up to the right shoulder.
- Lead aVL looks from the center of the heart up to the left shoulder.
- Lead aVF looks from the center of the heart down to the feet.
The first 3 limb leads (i, II and III) are also known as bipolar leads because they measure voltage directly between two electrodes. The augmented leads are unipolar because they use a single positive electrode and their negative reference is a combination of the other electrodes.
Chest leads
Chest leads look at the heart in approximately a horizontal plane. They are unipolar leads that use the average of all the limb electrodes as their negative (-) electrode. Each chest lead records electrical activity from the centre of the heart out towards one positive electrode.
- Lead V1 looks from the center of the heart to the V1 electrode, which is good for seeing right ventricular or septal problems.
- Lead V2 looks from the center of the heart to the V2 electrode, which is also good for right ventricular or septal problems.
- Lead V3 looks from the center of the heart to the V3 electrode, which is good for seeing anterior left ventricular problems.
- Lead V4 looks from the center of the heart to the V4 electrode, which is also good for anterior left ventricular problems.
- Lead V5 looks from the center of the heart to the V5 electrode, which is good for lateral left ventricular problems.
- Lead V6 looks from the center of the heart to the V6 electrode, which is also good for lateral left ventricular problems.
Extra leads
When you are trying to localise an infarct, it is sometimes useful to record extra leads by moving the electrodes to the right or posterior surface of the heart.
Right sided leads can be used to identify a right ventricular infarction. They are recorded by swapping one or more of the chest electrodes to the same position on the right side of the chest. The most common right sided lead is V4R.
Posterior leads can be used to identify a posterior ventricular infarction, by moving chest electrodes into new positions in the same horizontal plane as V6. These leads include V7, V8 and V9.
Rate

The rate measures the speed of the electrical heart beats. It can be described as normal, tachycardia or bradycardia.
In adults, a normal heart rate is usually 60-100 beats per minute. There should be 3-5 large grid squares between each beat.
Tachycardia is a rate that is faster than normal. In adults, a fast heart rate is usually over 100 beats per minute. There should be fewer than 3 large grid squares between each beat.
Bradycardia is a rate that is slower than normal. In adults, a slow heart rate is usually under 60 beats per minute. There should be more than 5 large grid squares between each beat.
Core Refs
- John Hampton and Joanna Hampton (2019) 2. The basics: the fundamentals of ECG recording, reporting and interpretation. The ECG Made Easy, 9th Edition (Book)
Grid squares
ECGs are normally printed on two different sized grid squares. They are recorded using a standard calibration to make comparison easier. These standard settings include a 'paper speed' of 24 mm/sec and 10mm/mV. This means that the grids they are printed on will represent a consistent time and voltage .
- The large grid squares represent 0.2 seconds each, so there will be 5 large squares per second of recording or 300 large squares per minute.
- The small grid squares represent 0.04 seconds each, so there will be 25 small squares per second of recording or 1500 small squares per minute.
Large squares rate
One of the fastest methods of calculating the rate is to count the number of large grid squares between two beats. If the ECG beats are regularly spaced apart and it was recorded at standard settings, you can find the rate by dividing 300 by this number.
Be careful: this method only calculates an approximate beat-to-beat rate. It can be misleading if the beats you choose are not representative of the overall rhythm, or if the beats are not regularly spaced apart.
Rhythm strip average rate
You can also calculate the average rate by using a longer strip of recording, such as the rhythm strip. For a 10 second length of recording, count the number of beats on this strip and multiply this number by 6 to find the rate in beats per minute.
This method is good for irregular rhythms such as Atrial Fibrillation or ectopic beats. These rhythms can also be described by using a rate range, e.g. Atrial Fibrillation at a rate of 120-160 bpm.
Challenge: Atrial rates
For some ECG rhythms the atria and ventricles may have different rates. In these cases it can be useful to calculate separate rates for the P waves and QRS complexes. The standard formulas still apply.
Challenge: Paediatric Rates
Paediatric patients have higher heart rates than adults. There are many slightly different published ranges, this is just one example.
- Neonates HR 100-180
- Toddler HR 80-110
- Preschooler HR 70-110
- School age HR 65-110
- Adolescent HR 60-90
Challenge: Rate at nonstandard calibration
At double speed calibration, the paper speed is 50mm/sec. The beats will appear twice as spread out as normal. The rate will also be double the normal rate, or 600/RR in large squares.
Half height calibration is sometimes used when the beats are so tall that they overlap eachother. This calibration setting does not affect the paper speed, so the rate will be calculated as normal.
Challenge: Rate variability
Some rhythm problems have clues in how the heart rate changes over time.
If there is a tachycardia with a sudden onset it may suggest that the rhythm is stuck in a loop called a re-entry circuit. By contrast, if the tacyhcardia has a more gradual onset it may suggest a gradual increase in stress or sympathetic tone such as fever or pain.
It is common for the rate to vary slightly over time, e.g. with respiration or position change, fever, pain, hydration or distress. If it remains a fixed rate that can also be a clue for an arrhythmia with a re-entry circuit.
Basic Rhythms

The rhythm describes the origin of each beat, in terms of whether it starts in the SA node (sinus), atria, AV node (junction) or ventricles.
Any rhythm can be described by 3 basic features: rate, regularity and QRS width.
Core Refs
- John Hampton and Joanna Hampton (2019) 2. The basics: the fundamentals of ECG recording, reporting and interpretation. The ECG Made Easy, 9th Edition (Book)
Regularity
Regularity describes how the beats are spaced apart. It can be regular, grouped, interrupted or irregular.
If the rhythm is regular, then the QRS complexes are evenly spaced apart.
If the rhythm is grouped, there will be regular groups of beats with gaps between them of different lengths.
If the rhythm is irregular, the QRS complexes will be unevenly spaced apart with no clear pattern.
QRS width
Another key feature of ECG rhythms is whether it is a narrow complex or wide complex rhythm.
Narrow complex rhythms have QRS complexes that are less than 100 msec wide (2.5 small squares at standard settings). Common narrow complex rhythms include Normal Sinus Rhythm, Sinus Tachycardia, Atrial Fibrillation and Atrial Flutter. These rhythms must originate from somewhere above the ventricles, because the only way to achieve a sharp narrow QRS complex is by travelling through the ventricles completely normally on the fast normal conduction highways.
Wide complex rhythms have QRS complexes that are more than 100 msec wide (2.5 small squares at standard settings). These wide rhythms can either start within the ventricles, or if they do start above the ventricles they must encounter a conduction block that prevents them from using the normal conduction highways through the ventricles. Examples of wide complex rhythms include Ventricular Tachycardia, SVT with aberrancy, or Bundle Branch Blocks.
Sinus rhythms
Sinus rhythms are a group of rhythms that all originate at the sinus (SA) node. They will all have a P wave before each QRS, and a QRS after each P wave.
Normal sinus rhythm has a rate of 60-100 beats per minute in adults.
Sinus tachycardia has a rate above 100 beats per minute in adults.
Sinus bradycardia has a rate below 60 beats per minute in adults.
A sinus arrhythmia appears the same as a normal sinus rhythm except its rate gets gradually faster then slower with each breath.
Fibrillation and flutter
Two common types of arrhythmias include fibrillation and flutter.
Fibrillation is chaotic, with the affected part of the heart all trying to depolarise from many different origins. This results in a quivering (fairly useless) part of the heart. Fibrillation can either affect the atria or the ventricles.
- Atrial Fibrillation is irregular with absent P waves. It is the most common sustained arrhythmia
- Ventricular Fibrillation is totally chaotic.
Flutter is a bit more organised than fibrillation, with regular flutter waves spreading out from the affected part of the heart. Flutter waves are usually very fast at about 300 beats / min.
- Atrial Flutter has regular flutter waves instead of P waves, which can make the baseline look like a sawtooth. Because the AV node normally can't conduct at this extremely fast rate, it usually only lets some of these impulses through to the ventricles.
Arrest rhythms
One situation where you need reliable and rapid rhythm interpretation skills is in a cardiac arrest.
There are 4 critical arrest rhythms where there may be no palpable pulse. These include VT, VF, PEA and asystole.
Ventricular tachycardia (VT) is a fast rhythm with wide QRS complexes. There are other things that can look like VT (e.g. bundle branch blocks) but in the setting of an arrest it may be safest to assume that a wide tachycardia like this is VT until proven otherwise.
Ventricular fibrillation (VF) is a chaotic disorganised rhythm.
Pulseless Electrical Activity (PEA) is a term that is used to describe any other rhythm that does not generate a pulse.
Asystole is a flat line with no electrical activity.
Of all the possible arrest rhythms, only the ventricular rhythms are shockable rhythms (i.e. VT and VF).
Axis

The cardiac axis describes the overall direction of ventricular depolarsiation. Think of it like painting a single arrow on the front of the chest. It can be described as normal, left, right or extreme axis deviation.
Core Refs
- John Hampton and Joanna Hampton (2019) 2. The basics: the fundamentals of ECG recording, reporting and interpretation. The ECG Made Easy, 9th Edition (Book)
The Hexaxial Reference System
The hexaxial references system is a model that can help to calculate the axis. It includes the direction of each of the 6 limb leads (hex = 6) in the frontal plane, measured in degrees clockwise from a horizontal line to the left.
- Lead I is horizontal (0°)
- Lead II is diagonal down to the left foot (+60°)
- Lead III is diagonal down to the right foot (+120°)
- Lead aVR is diagonal up towards the right shoulder (-150°)
- Lead aVL is diagonal up towards the left shoulder(-30°)
- Lead aVF is vertical (+90°)
There is a range of degrees for each axis variation.
- Normal axis: -30 to +90°.
- Right axis deviation: +90 to +180°.
- Left axis deviation: -30 to -90°.
- Extreme axis deviation: -90 to -180°.
Quadrants method
Once we know the directions of each limb lead, we can deduce the axis by using two simple rules:
- The axis is somewhere towards a positive lead.
- The axis is somewhere away from a negative lead.
The quadrants method uses lead I and aVF to calculate the axis because these two leads make convenient horizontal and vertical axes. However, because a normal axis range is slightly larger than one quadrant, we sometimes also need to look at lead II.
To use the quadrants method:
- Draw your axes, with lead I horizontal to the left and aVF vertical down to the feet.
- Check lead I:
- If it is positive, the axis is leftwards (towards I)
- If it is negative, the axis is rightwards (away from I)
- Check lead aVF:
- If it is positive, the axis is downwards (towards aVF)
- If it is negative, the axis is upwards (away from aVF)
- You should have only one quadrant remaining. If it is normal, right or extreme axis deviation you are finished. If it is somewhere in the left upper quadrant you will need to look at lead II to decide if it is normal or left axis deviation:
- If II is positive, the axis is somewhere towards lead II (+60), which makes it normal overall.
- If it is negative, the axis is somewhere away from lead II, which makes it left axis deviation overall.
Isoelectric method
The isoelectric method is a quick method of finding the axis if you can find an isoelectric lead. Look for a limb lead with QRS complexes that are equally positive and negative (isoelectric). The axis will be found perpendicular to the isoelectric lead in either a clockwise or anti-clockwise direction.
To use the isoelectric method:
- Draw all 6 limb lead axes on a chart
- Find the isoelectric lead. The axis will be 90 degrees from this lead in either a clockwise or anti-clockwise direction.
- Use your chart to find the perpendicular lead
- Check the perpendicular lead:
- If it is positive, the axis is directly towards this lead
- If it is negative, the axis is directly opposite this lead
Left axis deviation DDx
Left Axis Deviation can be caused by lots of things, including left ventricular hypertrophy, left bundle branch block, inferior MI, ventricular pacing, and others. The diagnosis of exclusion is a left anterior fascicular block.
Right axis deviation DDx
Right Axis Deviation is often caused by right ventricular hypertrophy, acute right heart strain (e.g. pulmonary embolism), COPD or other lung disease. It can also be caused by a lateral MI, hyperkalemia, dextrocardia, or just a tall thin patient. The diagnosis of exclusion is a left posterior fascicular block.
Extreme axis deviation DDx
Extreme axis deviation is usually due to a ventricular rhythm, but can also be due to hyperkalemia or very severe right ventricular hypertrophy.
It is important to know that an abnormal axis can be due to a simple electrode swap, especially if the axis suddenly changes between recordings when the leads are reconnected.
Challenge: Indeterminate axis
Occasionally the axis might be impossible to calculate because all of the limb lead complexes are the same (i.e. all isoelectric). We can call this an Indeterminate Axis. This can occur if depolarisation spreads through the heart from posterior to anterior such that there is no net movement in the frontal plane.
Challenge: Paediatric axis
In paediatrics, the normal axis varies with age. In general it starts out more rightward because the RV is more dominant. It becomes more leftward with age. Published normal ranges vary, e.g.:
- 1 month: +30 to +180°
- 1-3 months: +10° to +125°
- 3 months – 3 years: +10° to +110°
- Over 3 years: +20° to +120°
Axis deviation can be caused by congenital heart disease:
- Left axis deviation can be caused by AV septal defects, LV hyertrophy, or tricuspid atresia.
- Right axis deviation can be caused by RV hypertrophy.
- Extreme axis deviation can be caused by AV septal defects, tricuspid atresia, Ebstein anomaly, dextrocardia or Wolff Parkinson White syndrome.
Quality

ECG quality problems are so common that a quick quality check is essential for each ECG interpretation. This should include checking the patient's identity, ensuring the calibration is standard, looking for baseline artefacts and electrode misplacements.
Core Refs
- John Hampton and Joanna Hampton (2019) 2. The basics: the fundamentals of ECG recording, reporting and interpretation. The ECG Made Easy, 9th Edition (Book)
Standard settings
ECGs can only be compared easily if they are recorded at the same settings. The most common standard settings include a paper speed of 25 mm/sec and 10 mm/mV. These settings may be printed on the edge of the page, or there may be a calibration signal at the start of the trace that is a rectangle 5mm wide and 10mm tall (or some ECG machines record a very narrow calibration signal but write "25 mm/sec" separately).
Nonstandard calibration settings include double speed (50 mm/sec), where the trace will appear to be twice as spread out as normal.
Half height (5 mm/mV) is another setting that can make it easier to fit all the complexes on the page if they are very tall, but will not change the overall rate because the paper speed stays the same.
Machine interpretation
Unfortunately most automated ECG interpretation algorithms are frequently inaccurate. They are best treated with extreme caution, or disregarded. There are too many errors to count, but common ones include:
- Rate errors: counting tall T waves as extra QRS complexes, or not counting ectopic (extra) beats
- Rhythm errors: attributing many different rhythms to Atrial Fibrillation (not all that is irregular is AF), missing pacemaker spikes, mistaking artefacts for VT / VF, mistaking electrodes falling off for asystole.
- Interval errors: QT measurement can be inaccurate, especially with baseline artefact or U waves
- Baseline errors: any interpretation becomes dubious in the presence of baseline artefact
- Ischemia errors: automated interpretation will frequently miss signs of myocardial infarction and ischemia, or mislabel secondary ST or T wave changes as an infarct.
In general, the computer interpretation is better at calculating rate, intervals and axis, but worse at rhythm and ischemia interpretation. It also does not correlate the trace to the clinical context.
Baseline artefacts
Artefacts are caused by anything other than the heart's electrical activity. They include movement artefacts (e.g. muscles shivering, tremors, or tapping the electrode on purpose), other electrical devices (e.g. nerve stimulators, electrical beds) or electrodes being in poor contact with the skin.
One of the most important artefacts to be aware of is a chest compression artefact. It looks a bit like a very wide complex rhythm but it actually completely obscures the true underlying rhythm. This artefact prevents rhythm analysis while CPR is in progress.
One important clue to whether an abnormal ECG rhythm change is due to an artefact comes from looking across all of the leads. If the appearance is only in some of the leads, it is more likely to be an artefact as a true rhythm change should affect all simultaneously-recorded leads together.
Challenge: Electrode misplacement
Electrode misplacement is common, but can be hard to identify. Here are a few key patterns to recognise.
If you notice that Lead I has become a complete upside-down mirror image of normal then check the left and right arm electrodes. This pattern can be caused by accidentally putting the left arm electrode (LA) on the right arm and vice versa. Other limb lead reversals can be subtle.
It is very common to place the first two chest electrodes too high. If this has happened, the QRS complex may have developed evil bunny ears that can be easily mistaken for an incomplete right bundle branch block. The T waves in these leads may also become inverted and mimic a heart attack. This will all go back to normal if the ECG is repeated with the V1 and V2 electrodes in the 4th intercostal space.
Other chest electrode swaps can cause a bumpy ride in V1-V6. The chest leads should have a smooth progression where the QRS complex is mainly negative in V1 but becomes steadily more positive as you move through to V6. If an electrode is misplaced or swapped, this smooth transition may become interrupted.
There are many other subtle and not-so-subtle electrode misplacement errors. If in doubt, always check the electrode placement first!
ECG Basics
Feedback
This is an early prototype. How could it be improved?